

Thanks to Dr. Ramesh Dharawat for a discussion on two recent cases seen at SJGH. One patient presented with a pericardial effusion and the other presented with what was thought to be ventricular tachycardia.
Pericardial effusion
EKG: electrical alternans (click to view EKG from LITFL) due to “swinging” of the heart
Ultrasound/POCUS to see if the effusion is likely responsible for hemodynamic compromise
Look for RIGHT ventricular collapse and RIGHT atrial collapse as signs for tamponade
https://www.youtube.com/watch?v=QjqrO71mg0k (warning: this video plays loud classical music)
This video showcases RV collapse, similar the u/s Dr. Dharawat showed of the patient that presented to our hospital during morning report
Pericardiocentesis should NOT be routinely done for diagnostic purposes. Indicated for hemodynamic compromise as seen above.
Medication can lead to pericardial effusion as seen in the patient that presented to the hospital. Some medications implicated: hydralazine, minoxidil, procainamide. The patient was on minoxidil.
Article shared by Dr. Dharawat: https://www.omicsonline.org/open-access/understanding-minoxidilinduced-pericardial-effusion-2329-9517-1000323.pdf
Don’t forget to send pericardial fluid for cytology to eval for malignancy, especially in cases of tamponade
Article shared by Dr. Dharawat: https://www.nejm.org/doi/full/10.1056/NEJMicm1009066
Pericardial effusions are a frequent incidental finding on CT scans in sick hospitalized patients
Wide complex tachycardia: SVT conducted with aberrancy
Unstable = shock
At first blush, Figure A appears to be a wide complex tachycardia concerning for ventricular tachycardia (VT)
However, this is not VT. This is SVT conducted with aberrancy. Here’s some ways to help differentiate between VT vs. SVT conducted with aberrancy when you see a wide-complex tachycardia (WCT).
Rate in Figure A is unusually high for VT
Discordance in this EKG goes against VT (V5 and V6 are are discordant with V1-4). Concordance is when QRS in all precordial leads have the same pattern/direction
Old EKGs (see Figure B) show a BBB pattern showing the patient has a baseline prolonged QRS interval
This patient had SVT conducted with aberrancy and not VT. However, it is still important to assume VT in WCT until proven otherwise. It is helpful to check prior EKGs if the patient is stable. If unstable, use electricity.
Further reading: https://litfl.com/vt-versus-svt-ecg-library/

Figure A
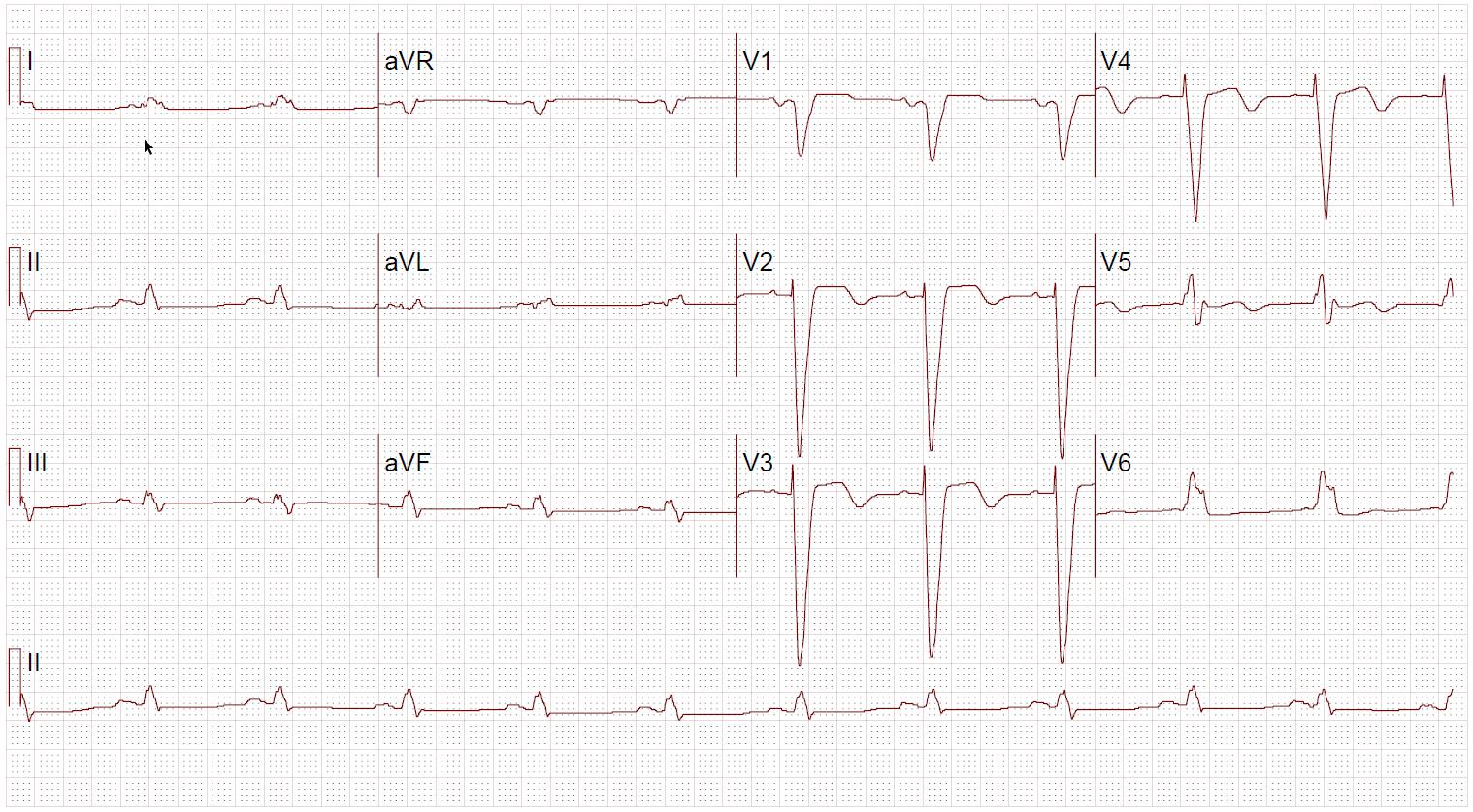
Figure B
References
U/s video: https://www.youtube.com/watch?v=QjqrO71mg0k
Electrical alternans: https://litfl.com/ecg-findings-in-massive-pericardial-effusion/
Save pearls to your Evernote: https://www.evernote.com/l/AbIj4fAIhkhJgrQswxrx_2DXufmMqlZ_noQ